Help! My Horse Roars! What is Laryngeal Hemiplegia?
Help! My Horse Roars! What is Laryngeal Hemiplegia?
Author: Fernanda Camargo, Animal and Food Sciences
Introduction
The larynx of the horse is part of the upper airway and serves as a conduit between the pharynx and the trachea, or the wind pipe that takes inspired air to the lungs for gas exchange. The larynx is comprised of a number of cartilages that work together to allow for increased airflow during exercise and to close the trachea during swallowing to prevent foreign material and food particles entering the trachea and consequently the lungs. The larynx is also where the vocal cords are located, and is therefore where the voice originates and is an instrument for phonation. The cartilages that comprise the larynx are: cricoid, thyroid, epiglottis, and the arytenoids.
During exercise, the arytenoid cartilages are held open (abduction) by the cricoarytenoideus dorsalis muscles, which are innervated by the recurrent laryngeal nerves.
Various ailments can affect the different parts of the larynx of horses. Diseases of the larynx can produce airway obstruction and sometimes dysphagia. Obstructive diseases, such as laryngeal hemiplegia, often produce an abnormal respiratory noise and, most important, they limit airflow, which leads to early fatigue and poor exercise performance.
For a video of a normal endoscopic examination of a horse, check out this video from Rood and Riddle Equine Hospital: https://www.youtube.com/watch?v=OLcqGW_Eo30.
What Is Laryngeal Hemiplegia?
Laryngeal hemiplegia is a condition in which one or both the arytenoid cartilages become paralyzed. Laryngeal hemiplegia is graded on a scale of 1 through 4, with 1 being the initial stages of the disease and 4 being complete paralysis.
For some reason, which has not been totally understood yet, the left side is generally affected more often than the right side or both sides. This condition is called idiopathic left laryngeal hemiplegia (ILH), a result of a progressive loss of myelin of the left recurrent laryngeal nerve. This condition results in a weakening of the muscles that abduct (open) and adduct (close) the arytenoid cartilages. The term idiopathic is used because the cause of the disease is unknown.
Certain genetic tendencies can predispose a horse to developing the disease. First, the left recurrent laryngeal nerve is longer and therefore more susceptible to trauma and failure than the right recurrent laryngeal nerve. Consequently larger horses with long necks are more susceptible to developing left laryngeal paralysis. Other possible causes of damage to the recurrent laryngeal nerve include: inflammation as a result of perivascular injection of an irritating substance intended for the jugular vein (the left vein is infinitely more used than the right vein for IV injections); trauma to the neck as a result of an injury or surgery of the neck; guttural pouch mycosis and other diseases of the guttural pouch; strangles abscesses; and pressure from tumors in the neck or chest.
Idiopathic laryngeal hemiplegia can affect a horse of any age, although foals are rarely affected. Large breed horses are more commonly affected than small breeds of horses or ponies. The progression of the disease occurs generally over a period of three to four months, although in some horses it can progress to complete paralysis in less than a month.
Idiopathic right laryngeal hemiplegia, as well as bilateral laryngeal paralysis, are uncommon, and therefore, if a horse presents with any of those, it needs to be fully examined by a veterinarian for the presence of other diseases such as guttural pouch mycosis, EPM, or organophosphate toxicity. Some horses with bilateral laryngeal paralysis may require an emergency tracheostomy, while others with less severe paralysis can breathe normally at rest but begin to have difficulty breathing with any type of activity or excitement, including attempts to perform an endoscopy.
Signs and Symptoms
The main clinical sign of laryngeal hemiplegia is a roaring sound during exercise, and exercise intolerance. Affected horses may have no symptoms at rest but start to roar as soon as the exercise demands a higher airflow through the larynx. Diagnosis is confirmed by client’s observations of the horse’s behavior and endoscopic examination. The veterinarian will close the nostrils of the horse to demand a big breath, at which point both arytenoids will abduct in a normal horse, and the affected arytenoid will be immobile or will abduct less on a horse with hemiplegia.
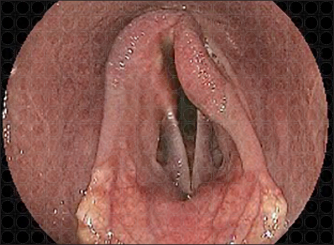
Photo courtesy of Dr. Michael Porter, PHD Veterinary Services, Alachua, Florida
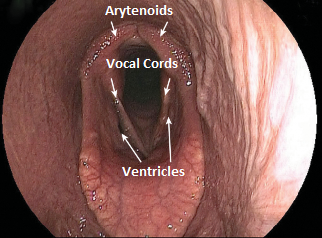
Photo courtesy of Dr. Michael Porter, PHD Veterinary Services, Alachua, Florida
How Do I Manage and Treat Laryngeal Hemiplegia?
A horse that develops inflammation to the recurrent laryngeal nerve and loss of abductor function on the affected side as a result of injury may regain function as inflammation subsides, but that will most likely happen within 30 to 60 days.
In those horses that do not respond to medical treatment, and in all cases of idiopathic laryngeal paralysis, the owner should consider surgical treatment once performance has deteriorated to the point where the horse is no longer useful for its intended purpose.
Surgical recommendations vary depending on the grade of hemiplegia, breed, age, and use of the horse. There are four surgical options, although laryngoplasty is by far the most common treatment.
- Prosthetic laryngoplasty is the most common procedure and is known as tie-back surgery. The paralyzed cartilage is “tied back” into an open/abducted position through an incision in the throat latch area.
- Ventriculectomy/cordectomy is a procedure in which the ventricle and the vocal cord are removed to widen the airway. It can be performed alone or along with a laryngoplasty. This procedure alone can improve performance and decrease roaring in horses that do not need to perform at high speed.
- Arytenoidectomy is not the first choice, as it is the removal of the paralyzed arytenoid cartilage altogether. This procedure is only done in horses that have already had a failed laryngoplasty. There is increased risk of complications due to aspiration, and decreased prognosis for returning to the previous level of competition.
- Neuromuscular pedicle graft is a procedure that includes the removal of a neck nerve (first cervical nerve) and the placement of this nerve in the muscle that abducts the arytenoid. Young horses with grade 3 hemiplegia are considered good candidates; grade 4 horses will not respond as well. Reinnervation takes 6 to 12 months. Horses that have had a previous tieback are not candidates for this procedure as they sustain damage to the first cervical nerve.
With some show horses, especially in hunters, the complaint may be the roaring noise instead of exercise intolerance. If the horse has diminished laryngeal function but still possesses considerable ability to open the left arytenoid (>70% abduction), the owner should be advised to wait until the situation deteriorates and there is further loss of abductor function before performing a tie-back because of reduced prognosis of the surgery in horses with some laryngeal muscle function. The main problem with waiting until the horse becomes more affected is that there is no predictable timetable for worsening with idiopathic laryngeal hemiplegia. The owner can also be given the option of continuing to compete the horse at a lower level until the horse becomes a more suitable surgical candidate.
The most commonly performed surgical treatment for left laryngeal hemiplegia in performance horses is prosthetic laryngoplasty. This procedure is usually performed through a laryngotomy incision or endoscopically, using a laser. A major benefit of the laser technique is that a laryngotomy incision is not required, which means some of the complications associated with a laryngotomy can be avoided and post-surgical care is simplified.
The degree of abduction needs to be sufficient to allow the horse to continue to perform. For example, in race horses, it is important to produce enough abduction (opening of the arytenoid) to allow the airflow required for sustained, high speed performance. In some horses the abduction produced by the laryngoplasty can lead to aspiration.
Other procedures, as cited above, may alleviate the roaring noise but not produce arytenoid abduction, and therefore, the airflow will continue to be less than optimal for a high performance horse. In horses with partial paralysis, there is often an initial improvement, especially with noise reduction, but as the disease progresses and paralysis becomes more complete, many of these horses will require a laryngoplasty.
Right laryngeal hemiplegia is treated in the same way as left laryngeal hemiplegia. The prognosis for right laryngoplasty is lower than that for left laryngoplasty simply because it is more difficult for a right handed surgeon to perform the surgery in a “back-handed” fashion.
Horses with bilateral arytenoid paralysis can be improved with a left tie-back. If the horse has difficulty swallowing and food material and saliva are entering the trachea, a permanent tracheostomy is a better option than laryngoplasty. Bilateral laryngoplasty is not recommended because of a greater risk for aspiration pneumonia.
In some horses the tie-back may not be successful, and the surgeon may wish to proceed to an arytenoidectomy, where the arytenoid will be resected instead of tied back. There are other surgical procedures that can be performed together or apart from laryngoplasty, and those will be the choice of the surgeon, according to his historical success rate with each procedure.
Care after the Surgery
In the first few days following laryngoplasty performed via an incision on the neck (close to the throat latch), most horses have some degree of difficulty eating and may have a mild fever. Water, saliva, and food particles may drain from the incision. Hay should be fed on the ground. This condition usually improves within days of surgery, especially with the administration of non-steroidal anti-inflammatory drugs. Some horses cannot tolerate the laryngoplasty and the aspiration of food, coughing, and inappetance become a threat to the horse’s health. In these horses, a second surgery is necessary in order to remove or loosen the laryngoplasty suture.
Following a laryngoplasty, the horse should receive 30 to 45 days of stall rest with hand walking only for exercise before resuming training. Hay and other feed should always be fed on the ground to reduce the chances of aspiration. Initially, most horses will cough intermittently while eating.
If horses continue to cough, it may be the result of a more serious and chronic aspiration problem. This condition usually occurs with horses whose arytenoids are over-abducted, but it can also happen to any horse after laryngoplasty. In addition, some horses develop a secondary problem with intermittent dorsal displacement of the soft palate while they are coughing. As training intensifies, there may be repeated episodes of fever as a result of low grade aspiration pneumonia. These horses will not have a great performance career.
Of all athletes, the racing horse is the most demanding because of the high volume of airflow required to compete successfully. The horse that has demonstrated the ability to race successfully before acquiring laryngeal paralysis has the best prognosis. Approximately 65 to 70 percent of these horses can be expected to return following laryngoplasty and race successfully. Unraced horses have a poorer prognosis because they may have other intrinsic issues that prevent them from racing successfully.
In most show horses, a successful laryngoplasty will eliminate any noise and the horse will be able to perform. However, in some horses, the surgery may have been successful in reducing or eliminating the abnormal respiratory noise, but the exercise intolerance persists because of inadequate abduction. In some horses, even after a successful laryngoplasty, the noise will return months or years after the surgery. In these cases, the owner may want to try a second laryngoplasty, or retire the horse.
Take Home Message
Laryngeal hemiplegia can happen to any horse as a result of an injury. Larger horses and those with long necks are more likely to develop the idiopathic form of the disease. Laryngeal hemiplegia can be corrected surgically with a high percentage of success. However, before performing any surgical technique on a horse, it is important for the owner to understand the chances for a successful career after the surgery as well as the amount of post-surgical care the horse will require. Generally, dissatisfied clients have not been made fully aware of the prognosis of the horse.
Video endoscopy should be performed on every horse being purchased as a high performance prospect because in many states sellers do not have to disclose previous surgeries to potential buyers.
References
The Merck Veterinary Manual. Laryngeal Hemiplegia in Horses.
http://www.merckvetmanual.com/mvm/respiratory_system/respiratory_diseases_of_horses/laryngeal_hemiplegia_in_horses.html.
Tetens, J., F.J. Derksen, and D.J. Hillman. Idiopathic laryngeal hemiplegia. Compendium on Continuing Education 23(1):2001.
Robertson, J.T., and N.G. Ducharme. Disorders of the Pharynx and Larynx. Equine Respiratory Diseases. International Veterinary Information Service. http://www.ivis.org/special_books/Lekeux/robertson/chapter.asp?LA=1.
